Description
Vocal intensity level (v.02.04)
Vocal intensity level (vocal IL) is one the key factors in clinical voice sound assessment. With the PHONANIUM script for measuring and showing vocal intensity level in the program Praat, all relevant aspects and statistics regarding (calibrated or uncalibrated) vocal IL can easily be obtained for different voice/speech tasks.
Author of the Vocal intensity level v.02.04 script
Youri Maryn
Included in this download
- Access to tutorial video with concise theory and illustration(s) on how to work with this Vocal intensity level script
- Access to tutorial video with concise theory and illustration(s) on how to calibrate intensity level measurements
- Access to tutorial video with concise theory and illustration(s) on how to evaluate the quality of sound recordings
- Access to tutorial video on how to work with the Personal information – New file script
- Access to tutorial video on how to implement/install plug-ins in the program Praat
- This plug-in
Plug-in details
Name of plug-in
plugin_PHONANIUM_VocalIntensityLevel_v.02.04
Content of plug-in
- Vocal intensity level v.02.04.praat: to determine several numerical data and graphs related to vocal IL with PHONANIUM’s script in the program Praat.
- setup.praat: to couple this script to a button in the dynamic menu of the program Praat.
- calibrationParameters.Table: a table in which previously and currently entered calibration data are stored. The last data set is used for calibration of the intensity levels measured in this script.
How to install this plug-in?
First, make sure to have downloaded and installed the program Praat (free available at www.praat.org) on your computer. Than download this plug-in.
Once downloaded, unzip the folder entitled plugin_PHONANIUM_VocalIntensityLevel_v.02.04 and place it in the following directory (i.e., the preferences directory of the program Praat), depending on your computer operating system and the name of the user (for example ‘Emiel’):
- Windows (Vista or later): C:\Users\Emiel\Praat\.
- Mac OSX: /Users/Emiel/Library/Preferences/Praat Prefs/. (However, sometimes the Library folder is hidden on a Mac OSX. If this is the case, you first open Finder, select the Go menu, and then press the alt key ⌥. While pressing the alt key ⌥, the Library becomes available as an option in the Go menu and can then be clicked/opened.)
- Linux: /UserName/.praat-dir/.
What is vocal intensity level?
As sound propagates as an ever-expanding energy sphere with the source at its center, its power per unit area or intensity decreases as distance from source (or radius from sphere) increases, according to the inverse square law. Intensity level refers to the intensity of a sound relative to a reference value (in dB). Vocal intensity level refers to the intensity level (IL) of vocal sound.
Although often presumed synonymous, vocal IL is not equal to acoustic power, sound volume or sound pressure. Loudness is another term that is often interchange with IL. However, whereas intensity level is a physically measurable element of sound, loudness is a perceptual attribute that is dominantly but not solely influenced by IL. Other factors are fundamental frequency and spectral properties of the sound signal (Baken & Orlikoff, 2000). In other words, intensity level relates to how sound there relatively is, whereas loudness refers to how much sound we here.
What determines vocal intensity level?
Vocal IL is regulated at different echelons in our speech system. The major factor is subglottal pressure, which controls the vocal intensity level below the vocal folds (Plant & Younger, 2000). The more pressure produced in the lungs, the higher the intensity level of vocal sounds: for every doubling in pressure above phonation threshold pressure there is an increase of 6 dB of vocal sound (Titze, 1994).
Glottal width and velocity of adduction are important factors at the level of the vocal folds. For every extra millimeter of glottal width there is an increase of 3 dB of vocal sound (Titze, 1988; Titze, 1994), and per doubling of speed of vocal fold closing there is an increase of 5-9 dB of vocal sound (Scherer, 2014). The relative duration within the glottal cycle with which the vocal folds are open/closed also influences the vocal IL: more closed quotient (or less open quotient) causes increase in vocal IL (Scherer, 2014), because there is more time to build up subglottal air pressure (Colton et al., 2006). From study in which laryngeal muscle activity was measured during silent, comfortable and loud phonation, level of vocal intensity was mainly associated with activity in the lateral cricoarythenoid muscle, but also with activity in the thyroarythenoid and cricothyroid muscles (Baker et al., 2001).
Above the vocal folds there are also factors that affect the intensity level of the speech signal. Shape and stifness of the supraglottal structures may influence the resonance charateristics of the vocal tract (Titze, 1994), and together with mouth opening this may govern the vocal IL.
However, all these factors do not operate in isolation. For example, glottal width and vibratory amplitude of the vocal folds increase with subglottal pressure. The influence each other to culminate in the final vocal IL.
Vocal intensity level as treatment outcomes measure
It is clear that vocal intensity level is related to/controlled by various physiological events in all layers of our peripheral speech system. Vocal IL can thus be considered as one of the most important acoustic features of the speech signal, and should therefore be taken into account of any clinical assessment of voice and speech.
Patients with unilateral vocal fold paralysis, for example, often lack the ability to phonate sufficiently loud. Their vocal folds cannot adduct adequately and lack tonicity and mass. This prevents building up sufficient subglottal pressure and consequently intensity of the phonatory sound (Miller, 2004). The speech of Parkinsonian patients is also typified by reduced vocal loudness (Fox & Ramig, 1997), and one of the main approaches in the treatment of their disordered speech is to focus on increasing vocal intensity level as stipulated in the Lee Silverman Voice Treatment (Ramig et al., 1995). Patients with muscle tension dysphonia and vocally traumatic behaviors, on the other hand, are often found to speak excessively loud (Altman et al., 2005; Van Houtte et al., 2009) because of raised phonatory effort.
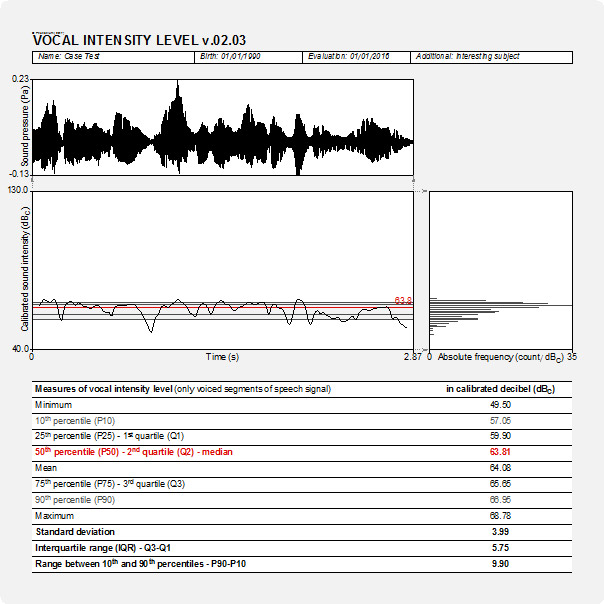
As abnormal vocal IL can be pathognomonic in several voie and speech pathologies, it is crucial to objectively measure it in clinical assessment and follow-up of larynx, vocal folds and speech in general. As such, vocal intensity level is one the key elements in documenting an individual’s voice/speech and in tracking outcomes of voice and speech treatment. With this PHONANIUM script for the program Praat, several descriptive statistics (i.e., minimum, maximum, 10th/25th/75th/90th percentile, median, mean, standard deviation, interquartile range, and range between 10th and 90th percentiles) of vocal IL become readily and rapidly available, as well as a graph showing its progression in time and and a graph displaying its absolute distribution. All this information can be collected on whatever speech task the clinician intends to analyze: steadily sustained vowel, spontaneous speech, read text, crescendo and decrescendo phonation, singing, diadochokinetic syllable repetitions, etc.
Phonanium’s script for vocal intensity level: specific features
Pre-analysis functions and formatting
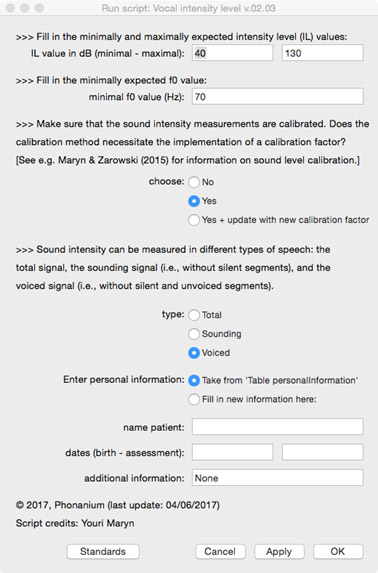
Before analyzing the voice/speech signal, the user is prompted in a form:
- to choose if an intensity level calibration factor is to be implemented, and if yes, which dB scale was used during the calibration procedure;
- to choose between the total signal/recording, the sounding signal (i.e., without silent segments) and the voiced signal (i.e., without silent and unvoiced segments);
- to enter personal information (i.e., name, date of birth, date of assessment and additional information) directly in this form, or to take this information after having it entered in the form of the Phonanium script entitled ‘Personal information’.
Graphical information output
- Oscillogram (sound wave)
- Sound intensity level in time
- Histogram of distribution of sound intensity level
Numerical/statistical information output in dB
- Minimum
- Maximum
- 10th percentile
- 25th percentile (or 1st quartile)
- Median ( or 50th percentile, or 2nd quartile)
- 75th percentile (or 3rd quartile)
- 90th percentile
- Mean
- Standard deviation
- Interquartile range
- Range between 10th and 90th percentiles
Important: calibration of vocal intensity level measurement
For clinical measurements of vocal intensity levels in the vocal range estimation to be reliable, it is essential to be calibrated before recording and analyzing sound signals (Ma, 2011). A straightforward method for calibration of the vocal intensity level has been described and found feasible, valid and accurate by Maryn & Zarowski (2016). This script automatically calibrates your intensity level measures when these data have been implemented/completed.
Click here to visit PHONANIUM’s page on vocal intensity level calibration.
Important: quality of sound recording
Many of the acoustic analyses and clinically relevant voice markers in the scripts of PHONANIUM imply sophisticated and complex procedures. However, when they are run on signals with bad recording quality, they loose their clinical value in terms of validity and reliability. So, prior to undertaking high-standard acoustic voice analyses, clinicians have to make well-considered choices in all of the following elements in the audio recording chain: room acoustics and ambient noise, type and placement of microphone, microphone preamplifier, and digital audio capturing device. To sample all relevant vocalizations and speech tokens as least polluted by recording-related noise as possible is what it essentially comes down to. For example Maryn (2017) offers an overview on how to deal with this.
Click here to visit PHONANIUM’s page on how to minimize recording-related influences on voice/speech signals.
Important: use the ‘Personal information’ script
With the script ‘Personal information v.01.02’ the user can complete an electronic form with the subject’s/patient’s name, date of birth, date of assessment, and optionally extra information. All this information (a) is than written into a table, (b) will be consulted by the other PHONANIUM scripts if the option “Take from ‘Table personalInformation’” is selected, and (c) will be written automatically in the output of these scripts. This increases the user-friendliness of working with PHONANIUM scripts in the program Praat, as the user/clinician has to complete this personal information only once during the entire voice assessment session.
Click here to visit PHONANIUM’s page on this ‘Personal information v.01.02’ script.
Disclaimer
For customers in the EU: this software currently has no CE certification. We are in the process of application. In the meantime, this software can be used for scientific as well as educational/learning purposes.
Program Praat
Click here to visit the website where the program Praat (Paul Boersma & David Weenink, Institute for Phonetic Sciences, University of Amsterdam, The Netherlands) can be downloaded. This software runs under the GNU General Public License. Click here to download this license.
References
Altman KW, Atkinson C, Lazarus C (2005). Current and emerging concepts in muscle tension dysphonia: a 30-months review. Journal of Voice, 19, 261-267.
Baken RJ, Orlikoff RF (2000). Clinical measurement of speech and voice. San Diego, CA: Singular Publishing Group.
Baker KK, Ramig LO, Sapir S, Luschei ES, Smith ME (2001). Control of vocal loudness in young and old adults. Journal of Speech, Language, and Hearing Research, 44, 297-305.
Colton RH, Casper JK, Leonard R (2006). Understanding voice problems. A physiological perspective for diagnosis and treatment (3rd edition). Philadelphia, PA: Lippincott Williams & Wilkins.
Fox CM, Ramig LO (1997). Vocal sound pressure level and self-perception of speech and voice in men and women with idiopathic Parkinson disease. American Journal of Speech-Language Pathology, 6, 85-94.
Ma EP-M (2011). Voice range profile: Phog. In Ma EP-M, Yiu EM-L (editors): Handbook of voice asessments, 253-267. San Diego, CA: Plural Publishing.
Maryn Y, Zarowski A (2015). Calibration of clinical audio recording and analysis systems for sound intensity measurement. American Journal of Speech-Language Pathology, 24, 608-618.
Maryn Y (2017). Practical acoustics in clinical voice assessment: a Praat primer. Perspectives of the ASHA Special Interest Groups SIG3 2017;2:Part 1.
Miller S (2004). Voice therapy for vocal fold paralysis. Otolaryngologic Clinics of North America, 37, 105-119.
Plant RL, Younger RM (2000). The interrelationship of subglottic air pressure, fundamental frequency, and vocal intensity during speech. Journal of Voice, 14, 170-177.
Ramig LO, Countryman S, O’Brien C, Hoehn M, Thompson L (1996). Intensive speech treatment for patients with Parkinson’s disease: short- and long-term comparison of two techniques. Neurology, 47, 1496-1504.
Scherer RC (2014). Laryngeal function during phonation. In Rubin JS, Sataloff RT, Korovin GS (editors): Diagnosis and treatment of voice disorders, 117-144. San Diego, CA: Plural Publishing.
Titze IR (1988). Regulation of vocal power and efficiency by subglottal power and glottal width. In Fujimura O (editor): Vocal fold physiology, volume 2. Vocal physiology: voice production, mechanisms and functions, 227-238. New York, NJ: Raven Press.
Titze IR (1994). Principles of voice production. Englewood Cliffs, NJ: Prentice Hall.
Van Houtte E, Van Lierde K, Claeys S (2009). Pathofysiology and treatment of muscle tension dysphonia: a review of the current knowledge. Journal of Voice, 25, 202-207.
Additional reading on vocal IL, perceived loudness and related issues
Behrman A (2007). Speech and voice science. San Diego, CA: Plural Publishing.
Kent RD, Read C (2002). Acoustic analysis of speech (2nd edition). San Diego, CA: Singular Publishing Group.
Kreiman J, Sidtis D (2011). Foundations of voice studies. An interdisciplinary approach to voice production and perception. Chichester, UK: Wiley-Blackwell.
Ma EP-M, Yiu EM-L (2011). Handbook of voice assessments. San Diego, CA: Plural Publishing.
Titze IR (2006). The myoelastic aerodynamic theory of phonation. Iowa City, IA: National Center for Voice and Speech.
Updates
Vocal intensity level (v.02.04), 27/01/2019
- Addition of a free field for the gender entry under ‘personal information’, to account for issues related to gender diversity.




Reviews
There are no reviews yet.